

Name has been changed to protect patient privacy. Clinical details and lab reports are shared with the patient’s consent.
A haemoglobin of 6.9 g/dL needs a moment of context. The reference range for women is 12.0 to 15.0. At 6.9, many women feel breathless walking up a single flight of stairs. Some struggle to stand through cooking a meal.
Chellammal was running a household on it. She was waking at 3 AM, attending a yoga class at 6, looking after a shop, caring for a pet dog, and going to bed at 11 PM on three to four hours of sleep. She is 49, a mother of two, and for about a year her periods had been arriving heavy and staying long, sometimes ten days of continuous bleeding.
This is the story of what one month of focused work did for her, and what it made possible next.
The Year Before She Came to Us
Chellammal’s troubles did not start the day she enrolled. Roughly a year earlier, during a particularly heavy episode, a blood test had shown her haemoglobin at 5.9 g/dL. That is severe anaemia by any definition. She was treated, the bleeding settled for a while, and life moved on.
But the pattern kept returning. Each cycle the bleeding would come heavy, and around day three she would start tablets to slow it. Some months she took them, some months she did not. She had also been taking daily Siddha medicines for about a year and a half, hoping things would gradually improve. Alongside the bleeding came leg stiffness, persistent fatigue, and the kind of tiredness that sleep never seemed to fix, partly because there was so little sleep to begin with.
If this pattern sounds familiar, it is because it is one of the most common stories of the perimenopausal years. We have written about why bleeding becomes heavy and unpredictable in perimenopause, and Chellammal’s case sits squarely inside that picture. What made her different was what finally brought her to us.
Her daughter had conceived naturally through our sister brand Fertilia’s program after failed IUIs. You may have read her story: Shalini, who conceived with endometriosis after two failed IUI cycles. Shalini is now in the pregnancy program, and her mother made a quiet decision: she wanted to be strong and well before her grandchild arrived. So she asked for help with her own health.
What the Work-Up Showed
When Chellammal enrolled in early May, we started where we always start: measurement, not guesswork.
Her baseline haemoglobin came back at 6.9 g/dL.

Her baseline report, 10 May 2026. Haemoglobin 6.9 g/dL against a reference range of 12.0 to 15.0.
The same blood draw answered a second question. Anaemia in a bleeding woman is usually about iron, but iron is not always the whole picture:
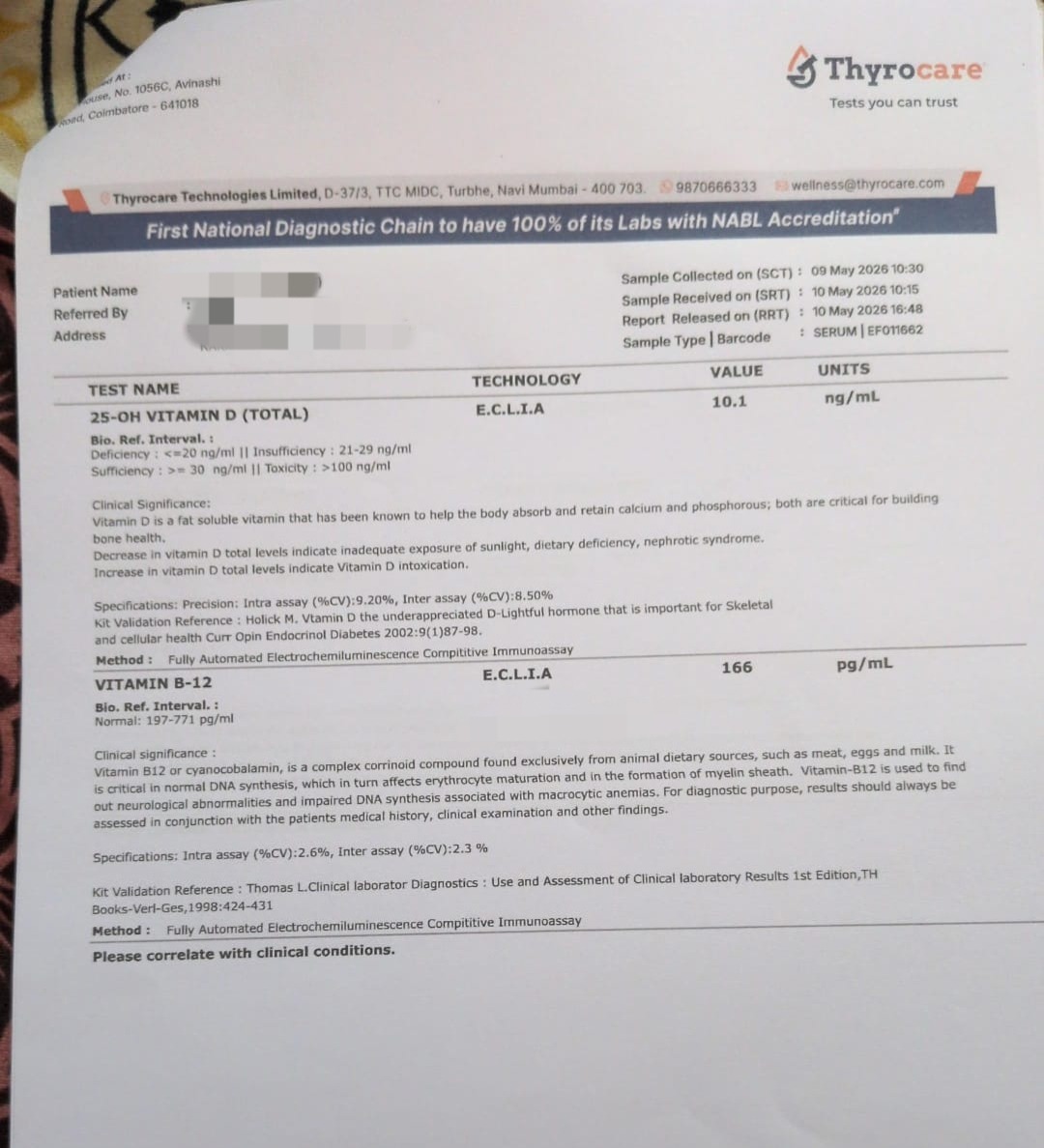
Vitamin D: 10.1 ng/mL (deficiency is 20 or below). Vitamin B12: 166 pg/mL (reference 197 to 771). Both deficient.
This mattered for her plan. Vitamin B12 is required to produce red blood cells. A woman who is iron deficient and B12 deficient at the same time rebuilds her blood slowly if only the iron is addressed. B12 deficiency is common in Indian women after 40, especially vegetarians, and Chellammal was a lifelong vegetarian.
Her pelvic ultrasound completed the picture:
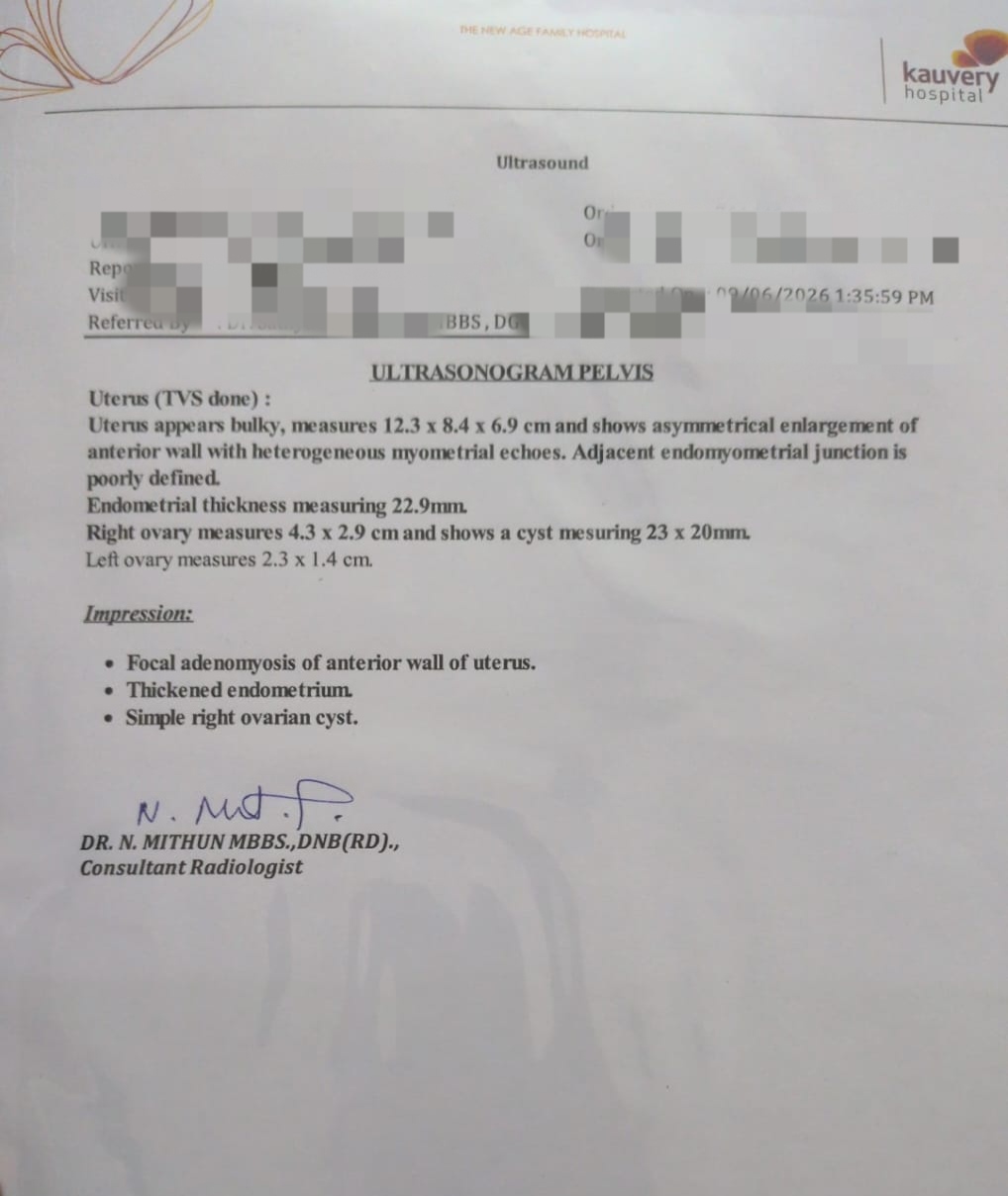
Her ultrasound: a bulky uterus with focal adenomyosis of the anterior wall, an endometrial thickness of 22.9 mm, and a simple cyst on the right ovary.
Adenomyosis is a condition where the uterine lining tissue grows into the muscle wall of the uterus, and it is one of the well-established causes of heavy, prolonged periods in the 40s. The thickened endometrium needed proper assessment too, which is standard practice at this age and with this bleeding pattern.
So an endometrial biopsy was advised. And here the story hit its wall.
The Biopsy That Had to Wait
With a haemoglobin of 6.9, Chellammal was told she would need a blood transfusion before the biopsy could be done safely.
That advice was sound. A procedure that can cause bleeding, performed on a woman whose blood count is already severely low, carries avoidable risk. Her doctors were protecting her.
But the word transfusion frightened her. For many women of her generation it carries a weight that is hard to describe: it sounds like the body has failed, like things have become serious in a way that cannot be walked back.
What I want you to notice is what she did next. She did not refuse the evaluation. She did not disappear, the way fear makes many women disappear from follow-up. She asked a different question: can I build my blood first?
That became the project of the next month.
The Plan
Her program rested on four pieces, each chosen for her specific situation:
1. Targeted supplementation. Iron, vitamin B12, and vitamin D together. Three deficiencies addressed at once, because correcting one while ignoring the others would have slowed everything down.
2. An iron-focused vegetarian meal plan she could live with. Chellammal is a complete vegetarian, though she was comfortable including eggs. Elakiya, our nutritionist, built her meals around that reality instead of fighting it: iron-rich greens (keerai), beetroot, dal, and eggs, paired deliberately for absorption.
3. Fixing the absorption leaks. Chellammal drank coffee in the morning and tea twice a day, often close to food. Tea and coffee contain tannins that blunt iron absorption, so her plan moved them away from meals and supplements. She also learned which foods help iron absorb better, and which quietly work against it.
4. Meal structure. She had no fixed meal times. She cooked and ate when hungry, which on a 3 AM start often meant long gaps and low fuel. Her plan gave her regular meal timing that fit around her yoga class and her shop.
Sleep was the fifth front. Three to four hours a night is its own health problem, affecting energy, cravings, and recovery. Sleep disruption in the perimenopausal years is something we work on gradually, and for Chellammal this work is still in progress. We mention it because real stories include the unfinished parts.
These are two of her actual plates from the program:

Greens cooked at home, boiled eggs for protein and B12, rice. Simple, repeatable, and built from her own kitchen.

Drumstick and carrot kuzhambu, beetroot poriyal, boiled eggs. Iron-supportive food that looks like a normal South Indian meal, because it is one.
Elakiya’s note from her file says more about the outcome than any lab value: “One thing that stood out about her was her consistency. She never missed her supplements and followed the dietary recommendations sincerely.”
💜 Living with heavy periods and constant tiredness in your 40s? There is usually a reason, and it can usually be worked on. Start a conversation on WhatsApp. No pressure, just guidance.
One Month Later
On 12 June, one month after her baseline report, Chellammal repeated her haemoglobin.
10.4 g/dL.
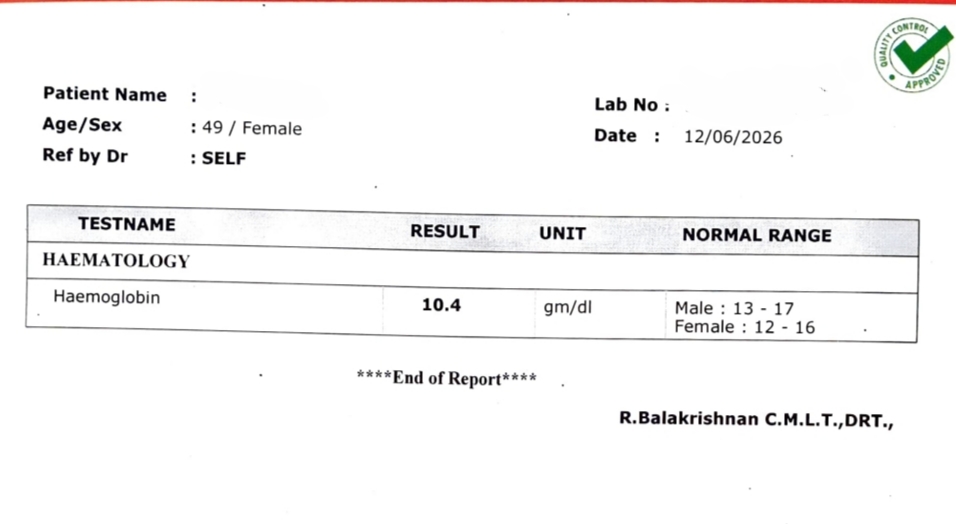
Her repeat report, 12 June 2026. Haemoglobin 10.4 g/dL, up from 6.9 one month earlier.

A rise of 3.5 g/dL in one month, on her own blood, with no transfusion. For perspective, a typical good response to consistent oral iron is a rise of about 1 to 2 g/dL over a few weeks. Her response was faster than average, and I credit two things for that: all three deficiencies were treated together, and she followed the plan with a consistency most of us would struggle to match.
Alongside the number, the day-to-day changes arrived:
- The bleeding became more manageable. Not gone, but no longer running her life.
- Energy returned. The drowsiness and the heaviness in her legs eased.
- And something less measurable. She told us she felt happy that she had done this for herself. After a year of treating her body as a problem to be silenced with tablets, she had watched it respond when it was given what it needed.
The Work That Remains
I want to be careful here, because this part is what makes her story trustworthy rather than just pleasant.
The adenomyosis has not gone anywhere. The thickened endometrium still needs assessment, and the biopsy that was advised remains advised. Those decisions sit with her gynaecological team, as they should, and we work alongside that care, never in place of it.
What changed is the ground she stands on. A month ago, the procedure needed a transfusion first, and the fear of that was enough to stall everything. Today she can walk into her evaluation on the strength of her own blood count, with her doctors making decisions from current numbers. Her body is ready for the next step. That is what this month was for.
If you take one thing from her story, take this: when a frightening medical step is in front of you, the choice is rarely between doing it immediately and avoiding it forever. Sometimes there is a third path, preparing your body so the step becomes safer, and that preparation is real medical progress, not a delay.
A Mother and a Daughter, Two Programs
There is a thread running through this story that we see more and more often. Shalini found us first, conceived through the Fertilia program, and moved into pregnancy care. Her mother watched the process up close, saw that it was unhurried and evidence-led, and trusted us with her own health.
Menolia is the perimenopause and menopause arm of my practice; Fertilia is the fertility arm. The same clinical team supports both. A family’s women often span both stages at once, and it is a particular joy to support a daughter preparing for a baby and a mother preparing to be strong for that baby, in the same months, under the same roof.
What Chellammal’s Story Tells Us
1. Severe anaemia can respond quickly when the whole picture is treated. Iron, B12, and vitamin D deficiencies overlap in Indian vegetarian women, and treating them together is what allows the bone marrow to do its work at full speed. Not every woman will see 3.5 g/dL in a month. Ongoing heavy bleeding, gut absorption issues, and the cause of the anaemia all affect the pace. But meaningful movement in weeks, not years, is a reasonable expectation with a complete plan.
2. Fear responds to a plan. Chellammal was afraid of a transfusion, and fear like that often ends in silence and missed appointments. What dissolved her fear was a concrete, dated path: supplements, meals, a repeat test in a month. If a procedure or report is frightening you into inaction, ask your doctor what can be done to prepare your body for it. It is a question doctors respect.
3. Vegetarian women can rebuild their blood. It takes more deliberateness: greens, dal, beetroot, til and dates on the plate, vitamin C pairings, tea and coffee moved away from meals, eggs if they are acceptable, and supplements to correct an established deficiency. Food sustains the recovery; supplements drive it. Her plates above are the proof that none of this requires exotic ingredients.
💜 If you are in your 40s, bleeding heavily, and tired in a way rest does not fix, a blood count and a scan can change everything about your next year. Message Dr. Suganya on WhatsApp. A short conversation is often where the next chapter starts.
Frequently Asked Questions
Is heavy, prolonged bleeding normal in perimenopause?
Heavy and irregular bleeding is common in the perimenopausal years because ovulation becomes erratic and the hormonal signals that limit the lining’s growth weaken. Common does not mean it should be endured. Bleeding that lasts beyond 7 days, soaks through protection hourly, or leaves you exhausted deserves evaluation, both to find the cause and to protect you from anaemia. Our full guide to heavy bleeding in perimenopause covers the causes and every treatment option.
How quickly can haemoglobin improve with supplements and diet?
With consistent oral iron and a supportive diet, a rise of about 1 to 2 g/dL over 2 to 4 weeks is a typical good response. Chellammal’s rise of 3.5 g/dL in one month was faster than average, helped by correcting her B12 and vitamin D deficiencies at the same time and by near-perfect consistency. The cause of the anaemia matters too: if heavy bleeding continues unchecked, it can offset what supplementation builds, which is why the bleeding itself must also be addressed with your doctor.
What is adenomyosis, and can it cause heavy periods?
Adenomyosis is a condition where tissue similar to the uterine lining grows into the muscular wall of the uterus, making the uterus bulky and tender and the periods heavy, long, and often painful. It is one of the most frequent findings behind heavy bleeding in women in their 40s. Diagnosis is usually by ultrasound, as in Chellammal’s case. Treatment ranges from medication to hormonal IUS to surgery depending on severity and your stage of life. Our Fertilia team has written a complete guide to adenomyosis.
Why would a doctor ask for a blood transfusion before an endometrial biopsy?
Safety. Any procedure on the uterus can cause additional bleeding, and in a woman whose haemoglobin is already severely low, even a modest loss can become dangerous. Asking for a transfusion first is protective, standard practice. Where the clinical situation allows time, raising the haemoglobin through aggressive correction of deficiencies is sometimes possible instead, as it was for Chellammal. That call always belongs to your treating team, made with your current numbers.
Can a vegetarian diet provide enough iron?
It can sustain healthy levels, with deliberate planning: greens like keerai and methi, dals, rajma, kala chana, beetroot, til, dates, and jaggery in moderation, paired with vitamin C sources like lemon or amla to improve absorption, and with tea and coffee kept an hour or two away from meals. Eggs, for women who accept them, add well-absorbed protein and B12. To correct an established deficiency, though, food alone is usually too slow, and supplements under medical guidance do the heavy lifting while diet holds the gains.
Do vitamin B12 and vitamin D matter for energy at this age?
Considerably. B12 is essential for producing red blood cells and maintaining nerves, and deficiency becomes more common after 40, especially in vegetarians. Low vitamin D contributes to fatigue, body aches, and long-term bone risk that rises steeply after menopause. Chellammal was deficient in both, and correcting them was part of why her recovery moved as fast as it did.
Does a program like this replace seeing a gynaecologist?
No, and Chellammal’s story shows the relationship clearly. Her scan, her biopsy advice, and her procedure decisions sit with her gynaecological team. Our program added the layer her medical care could not provide day to day: a personalised meal plan, supplement consistency, meal timing, and sleep work. The two together moved her from a frightening standstill to a safe next step. If your bleeding pattern has changed, these red flags tell you when to see a gynaecologist promptly.
Related Reading
- Abnormal & Heavy Bleeding in Perimenopause: A Doctor’s Guide
- Menopause & B12 Deficiency: Why It Rises After 40
- Menopause Fatigue: Why You’re Always Tired After 45
- Perimenopause Sleep Problems: Why You Can’t Sleep
- Menopause Red Flags: 8 Signs to See a Gynaecologist
- Menopause Calcium & Vitamin D: How Much & Best Foods
Every story we share on Menolia is real, verified, and shared with the patient’s explicit consent. Names and identifying details are changed to protect privacy.



